Legg-Calve Perthe's Disease
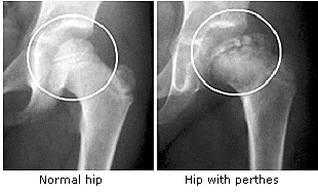
Image 41
- An avascular necrosis of the femoral head. Although LCPD can affect a wide age range of children, it is most commonly seen in children aged 5 to 8 years. The male-to-female ratio is approximately 5:1, and bilateral disease occurs in 10% to 15% of patients.
- Bilateral Perthes’ disease is usually metachronous; apparently synchronous bilateral Perthes’ should raise the suspicion of an alternative diagnosis, such as epiphyseal dysplasia.
- It is related to the changing pattern of the vascular supply to the femoral head during growth.
- The onset is insidious with painless limp and then development of hip, groin, lateral thigh, or knee pain. Physical examination will demonstrate leg length discrepancy, decreased abduction and internal rotation.
- Radiographic and sonographic diagnosis. There is a flattening and fragmentation of the femoral head and signs of joint effusion. Treatment is typically bracing or surgery
- The only abnormal radiographic findings for 4 to 6 weeks are those of synovitis: lateral displacement of the femoral head, widening of the medial joint space, and bulging of the lateral capsular fat or muscle planes. This is followed by the avascular state. The “dead” bone of the epiphysis is slightly sclerotic and smaller than its normal counter part.
- Many patients have delayed bone ages and appear to be younger than their chronologic age.
- In general, patients present with mild pain, a limp, and/or limited hip motion, which tends to have insidious onset.
- On physical examination, most patients have a mild limp and some may have a positive Trendelenburg sign. Additionally, thigh atrophy and limb length inequality may be measurable.
- The limitation of hip motion depends on the stage of the disease. Hip motion is generally good in the early stages, but hip irritability may be present because of synovitis, which can be persistent. Abduction and internal rotation are the earliest motions to decrease. In the fragmentation stage, hip motion can become severely restricted. Flexion and adduction contractures may develop in some patients. Motion improves during the reossification stage, but it can remain restricted by a severe residual deformity.
- Depending on the duration of the disease, thigh and calf muscle atrophy may be observed as well as limb-length discrepancy of 1 to 2.5 cm.
- Waldenstrom described four radiographic stages of LCPD according to the characteristic features of each: initial (increased radiodensity), fragmentation, reossification, and healed. Although radiography is useful in assessing disease progression, it lacks the sensitivity and specificity needed to demonstrate changes in vascular repair within the femoral head. Gadolinium-enhanced MRI can detect changes in bone perfusion in the early stages when radiographic changes are not apparent.
- The most common presenting complaint is that of insidious onset of a limp and mild hip or knee pain of several months duration. The pain is most often located in the groin region but up to 15% of patients report knee pain as the presenting symptom. The pain may be aggravated by physical activity; thus it may interfere with sports participation.
- The physical examination will usually reveal limited hip abduction and internal rotation which are thought to be secondary to muscle spasm.
- For Perthes’, both an anteroposterior and lateral or “frog leg” view (hips flexed and externally rotated) of the whole pelvis must be x-rayed. The anteroposterior view will show the more advanced changes of Perthes’-enlargement, flattening, sclerosis, or fragmentation of the epiphysis-but early changes such as the crescentic subchondral lucency, particularly in the anteromedial aspect (the site of maximal load bearing), are easily missed and best seen on the lateral view. In older children, slipped upper femoral epiphysis can be missed if the lateral film is omitted.
(6, 7, 8, 21, 23)