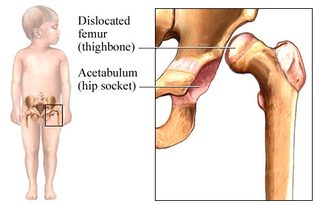
Developmental Dysplasia of the Hip
Developmental dysplasia of the hip (DDH)
- Occurs in approximately 1 in 1000 newborn infants. There are several risk factors that can increase the incidence. These risk factors include: breech presentation, family history of DDH, first-born status, and female gender.
- DDH has also been associated with other disorders such as metatarus adductus (hooked foot), torticollis, and congenital knee dislocation
- A hip examination for instability should take place for every newborn during the newborn examination as well as as at every well-check until the infant reaches 18 months old
- Congenital dislocation of the hip (CDH) due to developmental dysplasia is one of the more common pathological finding during routine examination of newborn infants. One of the most frequent findings of CDH is reduced or asymmetric abduction of the hips and is primarily composed of two elements -- instability and abnormal morphology
- Delayed diagnosis increases the risk of complications of treatment. Infants diagnosed after 6 months may require surgical correction.
- Late diagnosis can result in abnormal growth of the acetabulum, constriction of the anteromedial joint capsule, and contraction of the muscles around the hip. These problems may result in physiologic shortening of the musculature, leg length discrepancy, gait deviations, chronic pain and osteoarthritis.
- In addition to the Barlow and Ortolani Maneuvers, ultrasound may also be done to assess for DDH, however the reliability of this varies
- False positives tend to occur with the screening of DDH
Evaluation
- Infant examination begins with inspection in a relaxed state. In supine, remove clothing and diaper from the waist down and observe for symmetrical spontaneous movements of the hips. Evaluate for abduction to 75 deg and adduction to 30 deg which should occur without difficulty. Evaluate the Galeazzi sign by flexing the infants legs, with knees together, resting the soles of the feet on the table. A positive sign is unequal knee height, which may indicate unequal leg length. This test is sensitive after the first two months of life.
- In prone evaluate the gluteal folds for asymmetry and observe for any restriction in movement.
- The use of the Ortolani and the Barlow tests can assess for neonatal instability.
Image 22
(1, 4, 16, 25)
